

As the world grows richer and older, mental illness is becoming more common. John Prideaux considers the consequences
IT ALL BEGAN when she lost her head. According to legend, Dimpna, a 7th-century Christian heroine, fled her native Ireland when her father, mad with grief at the death of his wife, developed an incestuous passion for his daughter. The father came after the girl and, rebuffed once more, beheaded her in the flatlands of what is now northern Belgium. Dimpna was canonised, and in medieval Europe developed a reputation for divine intercession that could heal madness. Her cult centred on Geel, a small Belgian town that forms one point of a triangle with Brussels and Antwerp. By the 19th century Geel had developed a system of foster care for the mentally ill in which patients, or guests as they are referred to, are adopted by families. It continues to this day. When at the turn of the 20th century the Belgian government threatened its existence with a decree that the insane should live in institutions, the whole town designated itself as an asylum.
Geel’s system can make heavy demands on the host families. Not everyone is deemed suitable for a foster placement—a high suicide risk and a penchant for pyromania are two counter-indications—“but the list of exclusions is not so long,” says Bert Lodewyckx, who runs a team at the local hospital that looks after elderly patients. In a town of just 35,000 souls, about 270 families have people living with them who would otherwise be kept in an institution. Foster families are told nothing about the psychiatric history of their new companions. “For a time, being a foster family was prestigious, a bit like owning a Mercedes-Benz,” Mr Lodewyckx explains. Host families are paid about €20 a day, but their main motives are tradition and altruism.
The way the mentally ill are treated in Geel is unusual. At most times and in most places, caring for such people has been the responsibility of the biological family, which is not always kinder than strangers. Medieval Europeans sometimes locked up family members in basements or shut them away in pig pens. In China, where care of mental patients continues to fall largely on their families, such treatment is sometimes still being reported. In one case a man fashioned a homemade restraint for his son by fitting chains to a chair; in another a woman suffocated her sister with a pillow to lift the burden on the family.
China’s psychiatric system, such as it was, was largely shut down after 1949; the new Communist government made no provision for mental illness in a rationally ordered society. Yet as the country has grown richer and more urbanised, demand for mental-health care has grown. In 2012 China passed its first national mental-health law.
This is a typical pattern. The rise of psychiatry in America coincided with the post-war economic boom. Surveys by the World Health Organisation (WHO) show that spending on mental-health services increases sharply once GDP per person reaches around $20,000—the same level at which people start buying insurance, yogurt and other middle-class indulgences.
Two things lie behind this. Richer societies put more resources into diagnosing and treating mental illness, and older societies have more people with dementia. China is on its way to becoming both rich and old. This shift is usually accompanied by an expectation that society ought to shoulder more of the cost of treating mental illness, which can become too heavy for a single family to bear.
The statistical relationship between mental illness and development is new evidence for an old theory. Since the 19th century, people have been arguing that mental illness is a price to be paid for progress. In “Civilisation and its Discontents”, Sigmund Freud popularised the notion that neurosis increased in tandem with profit. Before Freud, an American neurologist, George Beard, had noted that a nervous disorder he labelled neurasthenia (and others nicknamed “Americanitis”) was on the rise. He put it down to the speeding up of modern life, facilitated by the telegraph, the railway and the press.
Neurasthenia disappeared from the psychiatrist’s lexicon in 20th-century America but enjoyed a long afterlife in China; Chairman Mao himself was said to suffer from the condition. It faded from view only after Arthur Kleinman, a Harvard anthropologist, conducted fieldwork in China in the 1980s and concluded that the symptoms of neurasthenia were rather like those of depression. Drug companies spied an opportunity to sell pills that they were already making. Rates of diagnosis for depression, which was virtually unknown in China 20 years ago, are now catching up with those elsewhere.
This is not because economic progress, of which China has seen more than any other country over the past three decades, makes people sick. Rather, it is due to a combination of the profound effect that growing richer has on diagnosis and the less forgiving standards for normal behaviour set by modern service-sector jobs. Dealing directly with customers makes different demands on the brain from work in a factory or on the land.
Surveys suggest that the incidence of serious mental illnesses such as schizophrenia (a condition characterised by hearing voices and withdrawal from society) and bipolar disorder (which causes extreme, uncontrollable mood swings) is fairly constant at between 1.5% and 3% of the population around the world. By contrast, the incidence of milder forms of mental disorder varies much more between and also within countries. This is true for common depression, anxiety, post-traumatic stress disorder, attention-deficit disorder and many others. In the rich world, these conditions taken together affect about 20% of the population at any point in time. America’s federal government estimates that in 2013 about 44m of the country’s population of around 325m suffered from some kind of mental illness, with depression and anxiety the most common.
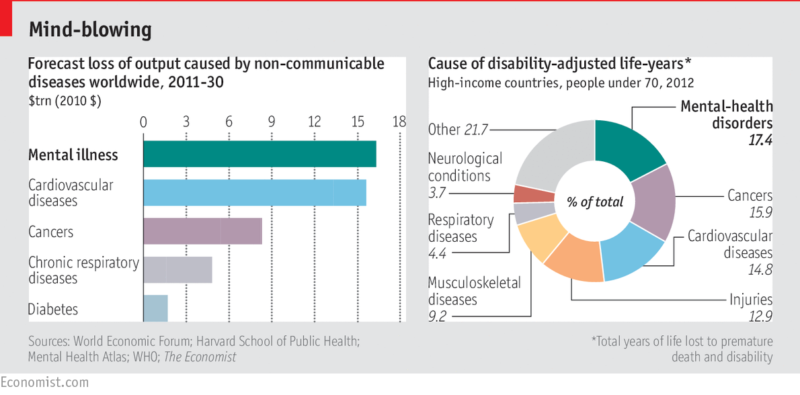
The OECD, a club of mostly rich countries, reckons that the direct and indirect costs of mental illness already exceed 4% of GDP in some places. A report from the Harvard School of Public Health and the World Economic Forum says that between 2011 and 2030 mental illness worldwide will cost over $16 trillion in output forgone (in 2010 dollars), more than physical ailments such as cancer, heart disease or diabetes (see chart). But such predictions should be treated with caution, for reliable numbers on mental illness, both within and across countries, are very hard to come by.
This is because, in the absence of a proper understanding of mental illness, the various disorders, syndromes and character traits that are labelled as such are really just thoughtful descriptions of changeable symptoms. In America, health-insurance companies rely on the definitions provided by the American Psychiatric Association’s Diagnostic and Statistical Manual (DSM) to determine what counts as sickness and what is merely within the usual range of variations from the norm. Each edition of the DSM removes some disorders and adds others. (The WHO maintains its own system, called the International Classification of Diseases, or ICD, whose definitions differ from the DSM’s.)
The most recent edition of the DSM lists around 300 mental illnesses. But the symptoms of mild depression are so different from the disabling effects of the severe sort that the two things probably ought not to share a name, and neither has much in common with, say, post-traumatic stress disorder (PTSD). This special report will try to make sense of this tangle by looking at the main afflictions of the brain at different stages of life. The first sort affects children as their brains develop; the second shows up in adolescents and younger adults; and the third appears as people get older and their brains begin to waste away.
Chasing a chameleon
The choice of definition, which is itself subject to change, has an effect on the diagnosis. But the thing doctors are trying to pin down is also inconstant. At the beginning of the 20th century it was common for people in the West to be diagnosed with nervous disorders. These have been replaced by conditions such as anxiety and depression. Soldiers in the first world war suffered shellshock, which could cause loss of the power of speech and, in some cases, partial paralysis, with no apparent physiological basis. By the middle of the 20th century other varieties of distress caused by battle had taken over. More recently PTSD has become an increasingly common psychiatric diagnosis for returning soldiers, displaying slightly different symptoms.
Symptoms change not only over time but from place to place. “To say that someone has a conduct disorder does not mean the same thing in Mozambique as it does in Manhattan,” says Shekhar Saxena, who runs the mental-health arm of the WHO. In some places hearing voices is considered normal, even desirable when part of a religious experience. In other it might be cause for prescribing antipsychotic medication. The difference is subjective: psychiatrists are usually interested only in voices that are distressingly insistent or say something unpleasant.
Other factors that affect the incidence of mental illness include people’s willingness to talk about it. Some might not want to admit that they are having problems. On the other hand, eligibility rules for welfare payments may provide an incentive for being diagnosed with anxiety or depression.
Diagnosis is also sensitive to advances in pharmacology. The current popularity of antidepressants, which are taken by one in ten Americans at any one time, has a lot to do with drug companies’ success in coming up with a form of drug delivery that is safe and does not have nasty side effects. Antidepressants that act on serotonin, a neurotransmitter that affects mood, have been around since the dawn of the jet age, but became widely used only once drugs such as Prozac, which were convenient and considered safe (and therefore easy for family doctors to prescribe) were developed. Until then, doctors had been fairly free with tranquillisers. In the 1950s Miltown, the brand name for meprobamate, a mild calming drug, was taken by about one in 20 Americans, mostly for anxiety.
The use of psychiatric medication itself sometimes seems like an epidemic in the rich world, but it can go down as well as up. In the late 1990s France was the world leader in malaise, with about 30% of its citizens taking psychiatric drugs, but since then the numbers have come down. Cognitive behavioural therapy, a form of short talking therapy that aims to break self-destructive patterns of thought and replace them with something more positive, has been found to work at least as well as pills for treating mild depression and is becoming more widely available.
Do not despair
Because mental illness is so hard to pin down and measure, it is easy to lose sight of how debilitating it can be. One widely used yardstick is the “Disability-Adjusted Life Year” (DALY), which the World Health Organisation defines as one lost year of “healthy” life free from physical or mental disability. Mental illness now accounts for a significant chunk of DALYs (see chart).
A more objective measure used in most health systems is the suicide rate. In Detroit, where a high murder rate, high unemployment and many abandoned houses meet any definition of a stressful environment, the Henry Ford Health System, which looks after much of the city’s population, has cut suicide among its patients by systematically assessing their risk.
In 2009, with the effects of the financial crisis still reverberating, the Henry Ford Health System managed to bring the number of suicides among its patients down to zero, an impressive achievement for an outfit that in 2013 counted 3.2m outpatient visits. There is no way of stopping those who are determined to kill themselves—“when someone is telling you that they want to make it look like an accident so their family gets the life insurance, then you know it’s really serious,” says Doree Ann Espiritu at Henry Ford. But many suicides are opportunistic acts of despair that can be prevented by putting netting under bridges, making it harder to jump onto subway lines and controlling access to large quantities of painkillers.
Because of the link between economic development, ageing and mental illness, the coming decades are likely to resemble an age of unreason. That is why Geel, which has been caring for people with such conditions for half a millennium, is worth paying attention to. What is striking about the town is how thoroughly normal it seems: the town square with its fake Irish pub; American pop music playing at a polite volume on the main shopping street. Mental illness, so often frightening, seems ordinary here. Geel’s system embodies principles for dealing with it—dignity, openness, kindness, patience—that should be embraced by societies everywhere.
Sources
Baron-Cohen, Simon, “The essential difference: Male and female brains and the truth about autism” (2004)
Congressional Budget Office, Rising demand for long-term services and supports for elderly people (2014)
Curry, John, Good news in the battle against military suicide, American Journal of Psychiatry (2015)
Frank, Richard and Glied, Sherry, “Better but not yet well: Mental health policy in the United States since 1950” (2006)
Goffman, Erving, “Asylums: Essays on the social situation of mental patients and other inmates” (1961)
Hayashi, Mayumi, “The care of older people: England and Japan, a comparative study” (2013)
Hinshaw, Stephen and Scheffler, Richard, “The ADHD explosion: Myths, medication, money and today’s push for performance” (2014)
Hogan, Michael et al., The president’s new freedom commission on mental health (2003)
Kleinman et al., “Deep China: The moral life of the person” (2011)
Moncrieff, Joanna, Efficacy of antidepressants in adults, British Medical Journal (2005)
National Institutes of Health, Recovery after an initial schizophrenia episode (research project, ongoing)
Nazeer, Kamran, “Send in the idiots: Stories from the other side of autism” (2006)
OECD, Making mental health count: The social and economic costs of neglecting mental health care (2014)
Phillips, Michael, China’s new mental health law: Reframing involuntary treatment, American Journal of Psychiatry (2013)
Porter, Roy, “Madness: A brief history” (2002)
Ramachandran, V.S., “Phantoms in the brain: Probing the mysteries of the human mind” (1999)
Silberman, Steve, “Neurotribes: The legacy of autism and the future of diversity” (forthcoming)
Styron, William, “Darkness visible: A memoir of madness” (1989)
World Health Organisation, Mental Health Action Plan (2013-2020)
World Health Organisation, “Mental health Atlas” (2011)
Yu-Tao Xiang et al., Mental health in China: Challenges and progress, The Lancet (2012)
From the Economist





